

Cupping Therapy
- Aug 23, 2016
- 46 min read
Wet cupping therapy (WCT) of prophetic medicine (Al-hijamah) is practiced in the Arabic medical literature where it is reported to treat many diseases differing in etiology and pathogenesis. Al-hijamah may be referred to as bloodletting cupping therapy or blood cupping therapy in medical studies and reports from Arabic countries. Both Chinese dry cupping therapy and WCT are partial steps of Al-hijamah. In this article, we review scientific principles, methodology, indications and therapeutic benefits of Al-hijamah in comparison with acupuncture and other types of cupping therapy. Scientific and medical bases of Al-hijamah were recently reported in the evidence-based Taibah mechanism (Taibah theory) where Al-hijamah is the only excretory treatment that clears blood, lymph and intercellular fluids from causative pathological substances (CPS).
Al-hijamah benefits from the histological structure of the skin in performing a percutaneous pressure-dependent and size-dependent non-specific blood filtration and excretion of CPS through the fenestrated skin capillaries upon application of negative pressure suction using sucking cups. Al-hijamah benefits also from the production of endogenous nitric oxide (vasodilator, antineoplastic and antimicrobial agent). Al-hijamah exerts many other health benefits e.g. enhancement of immunity and pharmacological potentiation. Al-hijamah was reported to clear blood significantly from serum triglycerides, total cholesterol, LDL-cholesterol, ferritin (circulating iron stores), uric acid, autoantibodies, cytokine receptors and others. Those therapeutic benefits may treat some diseases e.g. hyperlipidemia, hypertension, atherosclerosis, coronary heart diseases, gout, musculoskeletal pain conditions, hepatitis and iron overload conditions e.g. thalassemia. Importance of Al-hijamah may increase more in modern societies due to western diets and western life style. Therapeutic benefits of Al-hijamah are mainly related to the amount of excreted CPS not the amount of letted blood. Al-hijamah may carry some advantages better than acupuncture and other types of cupping therapy in treating a large number of diseases differing in etiology and pathogenesis.
1. Introduction
In modern medicine, there is no treatment modality that can purify both blood and interstitial fluids from noxious substances that are responsible for (or resulting from) disease pathogenesis. There is no physiological mechanism to excrete excess unwanted substances in blood (and interstitial fluids) that may disturb blood chemistry and physiological homeostasis causing different diseases e.g. high serum iron and ferritin in conditions of iron overload (e.g. thalassemia, hemochromatosis and bronze diabetes), high serum cholesterol, triglycerides and low density lipoproteins (LDL) in hyperlipidemia and atherosclerosis, high serum uric acid in gout and high interstitial fluid urate in gouty arthritis and others. Al-hijamah (cupping therapy of prophetic medicine) excretes all the above-mentioned noxious substances [1]. So, Al-hijamah may carry therapeutic benefits to all the above-mentioned medical conditions altogether. There is a bad need for using Al-hijamah in treating human diseases that are not responding well to current treatment modalities.
There is no pharmacological excretory treatment as all pharmacological treatments are introductory treatments needing careful study regarding possible precautions, drug-drug interactions, side effects and contraindications. However, some pharmacological treatments as iron chelation therapy may work to facilitate excretion of noxious substances e.g. excess iron in iron overload conditions. Excretory treatment modalities deserve more research attention as they may potentiate therapeutic effects of pharmacological treatments. Overcoming the language barrier through translating the national medical literature to medical English to be introduced to the international medical literature is of vital importance. Wet cupping therapy (WCT) of prophetic medicine (Al-hijamah) is practiced in the Arabic medical literature and is reported to treat many diseases differing in etiology and pathogenesis.
Better therapeutic effects and patients’ benefits may be gained when combining pharmacological treatments with excretory treatments e.g. cupping therapy. The need for Al-hijamah as a therapeutic modality increases more in the modern societies where the incidence of some diseases e.g. hyperlipidemia and hypertension increases. Al-hijamah may be referred to as bloodletting cupping therapy or blood cupping therapy in medical studies and reports from Arabic countries.
Cupping therapy is a term given to therapies using sucking cups (Figure 1) applied to certain skin areas for different therapeutic purposes. Suction applied to cups is an external factor that can be created and controlled according to the therapeutic indications [2, 3]. Cupping therapy is a simple, effective, economic, time-saving and synergistic line of treatment with pharmacotherapy. Cupping therapy has a deep-rooted history that is shared by different human civilizations. Dry cupping therapy (DCT) is a one-suction step technique (single S technique), where cups are applied to the skin for the purpose of sucking skin into cups. Moving the cups along the skin surface is described as moving cupping therapy.
FIGURE 1 : (Disposable sterile equipment for performing Al-hijamah are so simple. Disposable variable-sized plastic cups and a manual hand-help pump)
Traditional wet cupping therapy (WCT) is a two-step technique that involves scarifying skin superficially followed by cupping (suction using sucking cups) i.e. double S technique. Al-hijamah (WCT of prophetic medicine) is a three-step technique (suction, scarification and suction technique i.e. triple S technique) that is unique in its historical origin (Arabic in origin) and its steps that are still practiced in Arabic and Islamic countries [2, 3, 4].
Prophetic medicine is a term given to the medical knowledge gained from teachings, sayings (hadeeths), advices and deeds of prophet Muhammad peace be upon him related to health and disease treatment. [5]Recently, Loukas et al. reported that medical knowledge gained from Qur’an (spoken word of God) and hadeeths (spoken word of prophet Muhammad peace be upon him) can be an important source of humanity medicine in light of their astonishing agreement with modern medical knowledge [6].
2. Steps and Medical Bases of Al-hijamah
Prior to performing cupping therapy (including Al-hijamah), routine sterilization of the anatomical sites upon which cups will be applied must be done. Exact localization of those anatomical sites is critical to ensure success of the treatment plan. We recently reported the suitable anatomical sites for practicing Al-hijamah. [7]Sterilization is the first step and last step of cupping therapy. [3] Steps of cupping therapy differ according to the type of cupping therapy and the therapeutic indications. Single S cupping therapy (DCT) is a one-step cupping technique devoid of any excretory function i.e. only suction step with no skin scarification (Table 1). Double S cupping therapy (traditional Chinese WCT) has a single cupping (pressure-dependent filtration) step that achieves the excretory function. The step of opening the skin barrier (puncturing skin = scarification) is followed by the cupping step (Suction step = pressure-dependent excretion) i.e. double S technique [2, 3](Table 2).
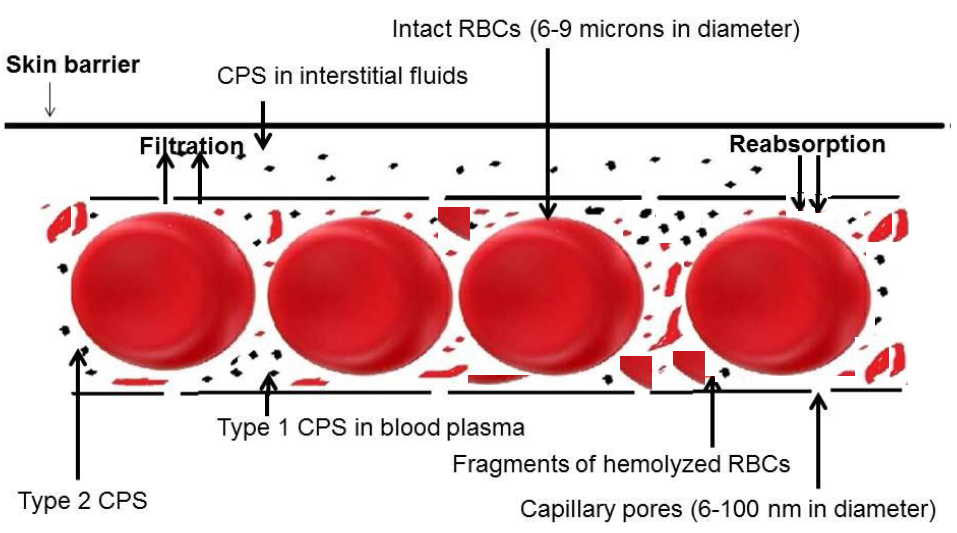
FIGURE 2 : (Disease conditions are mostly characterized by abnormal blood chemistry. Different causative pathological substances (disease-causing substances and disease-related substances) are present in the blood and interstitial fluids and cannot be excreted by physiological mechanisms e.g. excess serum iron and ferritin in thalassemia. Excretory modalities of treatment e.g. Al-hijamah help pharmacotherapy through excreting those pathological substances)
Al-hijamah combines both types of cupping therapy in a single original Arabic technique. [2, 3] Triple S cupping therapy (Al-hijamah) has three steps: cupping (suction step = pressure-dependent filtration of fenestrated skin capillaries beneath skin barrier), skin scarification (= shartat mihjam = small superficial multiple short openings of the skin barrier preceded and followed by a suction step) and second cupping (second suction step = pressure-dependent filtration of fenestrated skin capillaries and pressure-dependent excretion) i.e. pressure-dependent capillary filtration precedes and also follows opening the skin barrier during the triple S technique. [2, 3] Both Chinese DCT & WCT can be regarded as partial forms of Al-hijamah. [2, 3]Interestingly, the Chinese scientist Huang confirmed the difference in methodology between Chinese WCT and Arabic WCT (Al-hijamah). [4] Scientific and medical bases of Al-hijamah were recently reported in the evidence-based Taibah mechanism (Taibah theory) where Al-hijamah is an excretory form of treatment that clears blood, lymph and intercellular fluids from causative pathological substances (CPS) (Figure 1). [2, 3] El Sayed et al. confirmed the presence of many therapeutic benefits in Al-hijamah over Chinese WCT method [2,3] (Table 2). Al-hijamah is totally different from phlebotomy in which a pure blood loss occurs (Table 3).

FIGURE 3 : First technical step of Al-hijamah is first suction step. A. External negative pressure inside suction cups sucks skin into cups leading to formation of skin uplifting (skin dome). B. Inside skin uplifting, filtration of skin capillaries (pressure-dependent and size-dependent filtration and excretion) takes place. Collected fluids (filtered capillary fluids containing different causative pathological substances + collected interstitial fluids containing different causative pathological substances) start to accumulate inside the skin uplifting (skin dome) and approach the most superficial epidermal layer of the skin but cannot get out due to the presence of skin barrier. Small particles can be filtered through capillary pores and fenestrae while large particles (intact blood cells) cannot.
Table 1. Comparison between Traditional Chinese dry cupping therapy and Al-hijamah

Table 2. Differences between Al-hijamah and traditional wet cupping therapy

Table 3. Comparison between Al-hijamah and phlebotomy (fasd)


Figure 4. Taibah sign (A and B): At weak skin points of the skin uplifting (skin dome), skin vesicles (skin sacs filled with fluids) created by suction pressure may protrude through those weak skin points. Vesicles are filled with clear fluid (no blood cells as evidenced by absence of red color). Fluid inside vesicles is a fluid mixture (filtered fluid + collected interstitial fluids + CPS). Vesicles may result from increased suction pressure and or suction duration. Vesicles should be punctured using the sharp tip of a sterile scalpel. Application of local antibiotics or honey is recommended to promote healing in a sterile environment. Taibah sign is novel sign confirming Taibah mechanism for scientific bases of Al-hijamah (Taibah theory, named after Taibah city, Al-Madinah Al-Munawwarah in Saudi Arabia)

Figure 5. Second technical step in Al-hijamah is skin scarification (shartat mihjam) while third technical step is second suction. A. Skin scarifications (in Arabic: shartat mihjam) are small short superficial skin incisions (1-2 mm in length and 0.1 mm in depth). B. Skin scarifications open skin barrier for the excretion of collected fluids inside the skin uplifting (skin dome). Skin scarifications help transmission of second suction pressure to the inside of the skin uplifting (skin dome) to excrete collected fluids. Skin scarifications help transmission of second suction pressure to the inside of the skin uplifting around skin capillaries for more percutaneous capillary blood filtration. Skin scarifications cause a minor bleeding and loss of blood cells through the induced superficial skin incisions (scarifications). C. Criteria of shartat mihjam

Figure 6. Excretory function of Al-hijamah. A. Excretion of a bloody fluid mixture through the skin scarification sites inside the sucking cups. B. The excreted bloody fluid through skin scarification sites coagulates rapidly inside the sucking cups
Immediately after the first step in Al-hijamah, a fluid mixture (fluid barrier) is collected inside the skin uplifting (skin dome) between the superficial epidermal layers and dermal capillaries (Figure 3). This fluid mixture includes collected interstitial fluids, lymph, filtered capillary fluids with their CPS content. The collected fluids may protrude through weak skin points forming vesicles (Taibah sign) (Figure 4). All that will be excreted immediately upon skin scarification and second cupping (Figure 5), which causes a minor bleeding and loss of blood cells through the induced superficial skin incisions (scarifications). Cupped bloody fluid mixture starts to coagulate rapidly during putting cups for second suction (Figure 6). Immediately after finishing the cupping session, homeostasis is restored after clearance of blood and interstitial spaces from disease CPS (Figure 7). A transient post-cupping sign exists for few days and disappears without any sequelae (Figure 8). The negative pressure applied at the skin surface during cupping therapy is variable in strength according to the method of production of this negative pressure. Huber et al. reported that large pressure differences could be obtained when using different methods for inducing negative pressure. Huber et al. reported that the mean pressure produced was −200 ± 30 hecta Pascal (hPa) when using 2 cm flame, −310 ± 30 hPa with 4 cm flame, −560 ± 30 hPa with burning alcohol soaked cotton swab and −270 ± 16 hPa with rubber balloon. The pressure produced through rubber balloon was the easiest technically, moderate (not too high or too low) and was the most reproducible on repeating cupping practice as evidenced by reduction of the standard deviation by a factor of 2 compared to the flame methods [8]. The most superficial skin capillaries are fenestrated [9] (capillary pore size is 6-12 nm and fenestral size is about 60-80 nm) [10] allowing for capillary blood filtration when external suction pressure is applied (e.g. during Al-hijamah). As blood is a fluid composed of plasma (containing soluble constituents and CPS) and blood cells, suction pressure will filter small constituents (fluid and CPS having diameters in nm) not larger ones (cells having diameters in microns). When small skin scarifications (1-2 mm) are induced in skin barrier at skin uplifting during Al-hijamah, suction pressure will excrete collected fluids and filter smaller constituents (fluid and CPS) rather than larger ones (cells) i.e. there is a differential size-dependent filtration and excretion phenomenon (differential excretion phenomenon) occurring during Al-hijamah. Also, the rate of excretion is size-dependent i.e. smaller particles are excreted more rapidly than larger particles.

Figure 7. Restoration of homeostasis after complete or partial significant excretion of disease CPS. New interstitial fluid is formed by filtration at the arterial ends of capillaries and is reabsorbed at the venous capillary ends

Figure 8. Post-cupping sign: a transient skin uplifting surrounded by a circular depression occurs after cupping therapy and disappears without any sequelae within few days. Post-cupping sign is to be differentiated from other skin signs e.g. in purpura [3]
Most diseases are characterized by an abnormality in blood chemistry where a normal constituent may be high e.g. serum iron and ferritin in thalassemia or an abnormal constituent may be high e.g. serum autoantibodies in autoimmune diseases. Al-hijamah-induced non-specific clearance of the interstitial fluids and serum may normalize blood chemistry and restore physiological homeostasis through exerting multiple therapeutic functions (Table 4). The major therapeutic value in Al-hijamah over the Chinese WCT is the better blood clearance and excretion of the collected fluid mixture (containing CPS) through Al-hijamah as Al-hijamah is a two-step filtration process (suction pressure is applied twice), while Chinese WCT is a single step filtration process (suction pressure is applied once). [2, 3] This ensures better clearance of blood and interstitial spaces during Al-hijamah.
Table 4. Therapeutic health benefits of Al-hijamah N.B. Al-hijamah treats disease conditions through making use of one or more health benefits

Interestingly, a Saudi-Egyptian research group (Albedah et al.) searched the presence of evidence beyond using complementary and alternative medicine on PubMed, ACP journal club, Cochrane controlled trials register, Cochrane database of systematic reviews, Cochrane methodology register, database of abstracts of reviews of effects, health technology assessment database, Journals@Ovid, MEDLINE and the NHS economic evaluation database.
We agree with them regarding the presence of evidence regarding the validity of cupping therapy (including Al-hijamah) in treating pain conditions. However, it is advisable to differentiate the definition and methodology of Al-hijamah from traditional WCT and other types of cupping therapy when discussing the research results of both types of WCT and when interpreting the validity of Al-hijamah in treating different disease conditions. We agree with Albedah et al. in evaluating the therapeutic outcomes of WCT (both types) and in reaching the conclusion that WCT is effective for treating pain conditions.
However, regarding the therapeutic effects of cupping therapy in treating other disease conditions e.g. stroke rehabilitation, it was not clear which type of cupping therapy is meant by the conclusion drawn by the authors that the evidence is minimal. [11] Moreover, Al-hijamah treats predisposing factors for stroke progression e.g. hypertension, hyperlipidemia and others [1] and this is very important and beneficial for the patients regarding improving the current stroke condition and preventing future repeated stroke attacks. We may have a different opinion: first, it is advisable to differentiate research results of Al-hijamah (triple S technique) from research results of traditional Chinese WCT (double S technique) through comparing the methodology done and outcome of studies. Second, we hope if the authors in the future studies mention some details regarding these pain conditions or the rationale beyond their improvement. Third, we hope if they comment on cupping therapy regarding the type of treatment given and the beneficial effects of traditional WCT versus Al-hijamah in treating other diseases e.g. hypertension, fibromyalgia, headache, cellulitis, carpal tunnel syndrome, rheumatoid arthritis (RA), headache, migraine and others. [2] Fourth, we hope that the conclusion addressed by the authors sticks more to Al-hijamah rather than to other types of cupping therapy as research studies done in Al-hijamah are very few. Our understanding to the therapeutic benefits of Al-hijamah in light of future publications may expand the therapeutic spectrum of Al-hijamah in light of better understanding of its medical and scientific bases [2, 3, 7].
3. Therapeutic Benefits of Al-hijamah
Despite simplicity of the technique of Al-hijamah, many therapeutic benefits can be gained from it e.g. non-specific blood clearance, pain relief, pharmacological potentiation, restoring homeostasis and others. [2, 3] On the other side, there is no reported risk or harm that can be attributed to Al-hijamah. This confers many therapeutic advantages exerted by Al-hijamah over other conventional therapeutics. Table 4 lists some health benefits related to the practice of Al-hijamah. Nitric oxide (NO) is produced endogenously in enormous amounts as a response to skin injury [2, 12, 13]. (e.g. skin scarifications occurring during Al-hijamah). Interestingly, NO is the functional metabolite of some widely used drugs e.g. nitroglycerine for treating coronary artery ischemia (through inducing coronary dilatation) and sodium nitroprusside for treating severe hypertension. Sodium nitoprusside acts as NO donors. [14] Nitroglycerine and sodium nitroprusside were reported to have powerful actions to dilate blood vessels e.g. the radial artery. NO was reported to induce a decrease in the pressure wave reflection and systolic blood pressure better than phentolamine (α-adrenergic antagonist), verapamil (calcium-channel antagonist) and hydralazine (arterial vasodilator) [14].
4. Al-hijamah as a Pharmacological Potentiator
Al-hijamah was reported to have excellent therapeutic effects when it was used as a sole treatment [15] and as a combined treatment with conventional pharmacological treatments. [16] Many disease conditions responded better to Al-hijamah than to conventional pharmacological treatments. [15, 16, 17] However, Al-hijamah is not a substitute for pharmacological treatments. Instead, Al-hijamah may act as a pharmacological potentiator. Pharmacological potentiation is the sole target of drug combinations when treating various diseases and aims at gaining synergistic therapeutic effects via making benefits of combining more than one drug acting through more than one mechanism of action. It aims also at decreasing drug dose, frequency of drug administration and possible side effects. Contrary to that is drug-drug antagonism due to both chemical and pharmacological interactions where one drug decreases pharmacological actions and therapeutic effects exerted by another drug. Being a non-chemical and non-pharmacological therapy, Al-hijamah does not have any antagonistic effects with any therapeutic drug or pharmacological treatments. Moreover, Al-hijamah was reported to exert pharmacological potentiation with pharmacological treatments for treating many diseases e.g. RA [16] and headache [15]. Al-hijamah removes CPS from the site of pathology (whether the pathology is localized or generalized), from blood and from interstitial fluids. This enables pharmacological treatments to do better against a lower concentration of CPS, which prepares the site of pathology for a better response to administered pharmacological therapeutics. This may give a better chance for the immune system and homeostatic mechanisms to do better. [15, 16, 17] Sahbaa et al. reported that combination of bloodletting WCT (Al-hijamah) with anti-rheumatoid drugs was synergistic and did better than the mere use of conventional anti-rheumatoid drugs. [16] They reported also that conventional anti-rheumatoid drugs (e.g. methotrexate) induced a significant decrease in white blood cell count (bone marrow suppression) whereas combined therapy (Al-hijamah plus methotrexate) induced leukocytosis. [16] Moreover, the count of natural killer cells significantly decreased with conventional therapy and significantly increased with combined therapy. [16] In RA, soluble interleukin-2 receptors (SIL-2R) is strongly correlated with disease progression, pain intensity (measured by visual analogue scale, VAS), tender joint count (TJC), swollen joint count (SJC), disease activity scores (DAS) and laboratory markers of disease activity e.g. erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and rheumatoid factor. [16] The authors reported that combined therapy resulted in a significant reduction in concentration of SIL-2R over three successive months of treatment compared to base line levels while there was no significant reduction when conventional therapy was used. [16] Improvements occurred in a time-dependent manner [16].
Moreover, Ahmadi et al. reported that when treating patients suffering from migraine headache with Al-hijamah, clinical improvements were recorded in the form of reductions of the mean headache severity, duration (in days) of headache and frequency of medication administration [15].
5. Therapeutic Indices of Al-hijamah
To evaluate and quantitate the therapeutic benefits gained after performing Al-hijamah, many novel therapeutic indices of Al-hijamah can be calculated. Being novel determinants for the efficiency of Al-hijamah, therapeutic indices evaluate the technique done, practitioner’s skills and patient’s response to treatment and may help future follow-up of treatment. Therapeutic indices of Al-hijamah include excretion value, purification index, pharmacological potentiation index, immunological index and clinical therapeutic index.
6. Excretion Value
Excretion value (EV) is the quantity of CPS excreted after the end of the session of Al-hijamah. EV can be calculated from the formula: EV= (Initial concentration of any substance in serum before Al-hijamah in concentration unit/blood volume unit) - (concentration of the same substance in serum after Al-hijamah in concentration unit/blood volume unit). EV should be performed within the first 24 hour after Al-hijamah.
Clinical importance of EV comes from quantitating the efficiency of Al-hijamah in excreting a substance from serum i.e. pure excretory function of Al-hijamah. EV can judge the best hand skills among different practitioners of Al-hijamah depending on comparing the excretory effects of Al-hijamah. As EV can be affected by many variables of Al-hijamah technique e.g. anatomical sites for practicing Al-hijamah, pressure inside cups, time for cups application, number of skin scarifications and others, EV can be used to standardize Al-hijamah by choosing the best of those variables in light of future research.
As a practical example, Sahbaa et al. [16] treated RA with Al-hijamah where they reported a decrease in serum level of some CPS related to the pathogenesis of RA. In the patients’ group who received combined treatment (Al-hijamah and pharmacotherapy), rheumatoid factor decreased from 131.47 IU/ml to 51.54 IU/ml (Table 5). This means that EV for rheumatoid factor is (131.47 - 51.54 = 80.02 IU/ml) while EV for SIL-2R is (2023 – 1790 = 233 pg/ml).16 In another practical report in healthy subjects, the author reported a significant decrease in serum uric acid, ferritin, total cholesterol, LDL-cholesterol and triglycerides after Al-hijamah for healthy subjects. EV for uric acid was (4.5-3.7= 0.8 mg/dl), EV for total cholesterol was (158-136.3 = 21.7 mg/dl), EV for serum triglycerides was (164.9-119.8 = 45.1 mg/dl), EV for LDL-cholesterol was (71.8-55.1=16.7 mg/dl) and EV for ferritin was (129.4-100.6 =28.8 ng/ml) [1].
Table 5. Therapeutic benefits exerted by Al-hijamah in treating rheumatoid patients by Sahbaa et al. [16] N.B. Group I: Patients who received conventional pharmacotherapy for RA; Group II: Patients who received conventional pharmacotherapy for RA + Al-hijamah

7. Purification Index (Clearance index) of Plasma
Purification index (PI) is the percentage purification of plasma from any CPS component estimated at different time points after Al-hijamah.
PI can be calculated from the formula: PI= 100 X [(Initial concentration of any substance in serum before Al-hijamah ̶ concentration of the same substance in serum after Al-hijamah)/ initial concentration of same substance in serum before Al-hijamah]. PI should be measured at many time points after Al-hijamah. Clinical importance of PI is that it correlates the clinical improvements seen after Al-hijamah with the degree of serum clearance from a given CPS. PI can judge the pharmacological potentiation effect when comparing the effect of pharmacological treatments combined with Al-hijamah versus pharmacological treatments only in decreasing the serum concentration of a noxious substance. PI estimates the rate of re-accumulation of a given CPS at different time points, which will facilitate estimating the proper time for performing the next session of Al-hijamah. PI measures also the combined therapeutic benefits of the excretory, immunological and pharmacological potentiation effects of Al-hijamah.
Taking Sahbaa’s report [16] as a practical example, PI for rheumatoid factor = [100X (131.47 - 51.54/131.47)] = 42% i.e. one month after Al-hijamah, patients’ serum was cleared from about 42% of its initial rheumatoid factor concentration before treatment. Serum clearance increased further to 60.8% after the second month of treatment (Table 5) and increased to 79.9% (Table 5) after the third month of treatment. PI for SIL-2R was [100X (2023 - 1790/2023)] = 11.5%.
In the second above-mentioned practical report, [1] PI for uric acid was [100X (4.5-3.7)/4.5] = 17.78%, PI for total cholesterol was [100X (158-136.3)/158)] = 13.7%, PI for serum triglycerides was [100X (164.9-119.8)/164.9] = 27.3%, PI for LDL-cholesterol was [100X (71.8-55.1)/71.8]= 23.2% and PI for ferritin was [100X (129.4-100.6 =28.8 ng/ml)] =22.2%. [1] Based on that, Al-hijamah (as a single session or multiple sessions) may be efficient as a therapeutic modality against the risk factors for developing coronary diseases, atherosclerosis, gout, iron overloading conditions e.g. thalassemia and others. Interestingly, unlike Al-hijamah, traditional WCT was reported to be not significant in improving risk factors of coronary heart disease where the lipid profile status did not differ significantly between the patients who received dietary advice alone and those who received dietary advice combined with WCT. [18] In a similar issue, Al-hijamah was reported to decrease serum ferritin level (circulating iron stores) significantly, [1] which strongly recommends Al-hijamah as a promising treatment for anemic diseases characterized by iron overload e.g. thalassemia. More interestingly, Al-hijamah does not induce a significant blood loss, which keeps the red cell mass and hemoglobin level within the normal range [19]. On the other hand, excessive WCT (in multiple number of sessions or amount of bloodletting) reduced serum iron maximally and induced iron-deficiency anemia. [20, 21]This may confirm superiority of Al-hijamah over traditional WCT as Al-hijamah is a filtration-dependent excretory procedure (that excretes disease CPS) rather than a bloodletting technique [2, 3] i.e. Al-hijamah does not cause excessive blood loss. Al-hijamah was reported as the only form of cupping therapy to treat viral hepatitis where Al-hijamah reduced hepatitis C virus RNA load from (3.52 ± 0.53) (X 105 IU/ml) to (2 ± 0.38) (X 105 IU/ml). There was a seroconversion from positive PCR to negative PCR in 10% of cases This means that Al-hijamah cleared patients’ blood from hepatitis viruses (through both excretory and immunological functions of Al-hijamah) by about 43.18% [22, 23].
8. Pharmacological Potentiation Index
Pharmacological potentiation index (PPI) measures the degree of pharmacological potentiation when combining Al-hijamah with conventional pharmacological treatments versus the mere use of conventional pharmacological treatment. PPI records the best drug combinations to be administered with Al-hijamah. PPI= [100 X (Therapeutic effects of Al-hijamah + conventional pharmacological treatments)/ (Therapeutic effects of conventional pharmacological treatments only)].
Taking Sahbaa’s report [16] as a practical example (Table 5), PPI for improving pain intensity was [100 X (7.8-5.6)/(8-7.1)] = 244.4% i.e. combination of Al-hijamah with conventional treatments for RA increased pharmacological potency of conventional pharmacotherapy treatments by 244.4%. Moreover, PPI for decreasing serum rheumatoid factor was [100 X (131.47-51.46)/(129.75-122)] = 1032%.
9. Immunological Index
Immunological index (II) measures the degree of immunological response to Al-hijamah whether the response was a decrease in pathological immunity (e.g. autoimmunity) or an increase in natural immunity e.g. leukocytosis and lymphocytosis. II= [100 X (Immunological response after Al-hijamah)/(Immunological response before Al-hijamah)].
Taking Sahbaa’s report [16] as a practical example (Table 5), II for induction of leukocytosis = [100 X (10.05/ 6.94)] =.156% i.e. natural immunity (using leukocytosis) increased by 156% after combination of Al-hijamah with conventional pharmacological treatment. Moreover, II for increasing natural killer lymphocytes was [100 X (11.33/ 8.5)] =.133% i.e. natural immunity using NK cells increased by about 133% after Al-hijamah.
10. Clinical Therapeutic Index
Clinical therapeutic index (CTI) is the percentage improvement of a tested clinical parameter (e.g. pain intensity, disease activity, blood pressure value and others) after Al-hijamah (as a sole treatment or as a combined treatment) measured at different time points. CTI can be calculated from the formula: CTI = [100 X (clinical parameter before Al-hijamah ̶ clinical parameter after Al-hijamah)/ clinical parameter before Al-hijamah]. CTI should be measured at many time points after Al-hijamah. CTI can evaluate the clinical therapeutic efficacy of Al-hijamah for treating a given disease. CTI can correlate PI with the clinical outcome after Al-hijamah. CTI can quantitate the percentage of clinical improvement at different time points and estimate the longevity of improvement after one session of Al-hijamah and compare the degree of synergism with pharmacological treatments. CTI may record occurrence of any side effects or any signs of malpractice.
Abd al-Jawad et al. [24] reported a significant statistical improvement in clinical indices in asthma patients when combining Al-hijamah with asthma pharmacotherapy better than asthma pharmacotherapy as a sole treatment. Reported improvements included daytime symptoms, nocturnal symptoms, need for reliever, exacerbations, eosinophil cationic protein, peripheral esinophilic count and improvement in respiratory function tests (from 25%-75%) [24].
Taking Sahbaa’s report [16] as another practical example (Table 5), CTI for improving pain intensity (measured by VAS) is [100 X (7.8-4.7)/7.8] = 33.8% one month after performing Al-hijamah combined with conventional treatment i.e. pain intensity decreased by 33.8% one month after treatment then decreased by [100 X (7.8-5.16)/7.8] = 39.7% two month after treatment and finally decreased by [100 X (7.8-3.2)/7.8] = 58.9% three months after treatment. Moreover, CTI for improving TJC in rheumatoid patients treated by combined Al-hijamah with pharmacological treatments (within the same time period) was 42%, 50 and 75.7%, respectively. CTI for improving SJC in rheumatoid patients treated by combined Al-hijamah with pharmacological treatments (within the same time period) was 32%, 53.8 and 77.8%, respectively. CTI for improving ESR in rheumatoid patients treated by combined Al-hijamah with pharmacological treatments (within the same time period) was 7.8%, 12.1 and 21.6%, respectively. CTI for improving CRP values in rheumatoid patients treated by combined Al-hijamah with pharmacological treatments (within the same time period) was 42%, 60 and 77%, respectively.
11. Therapeutic Indications and Diseases Reported to be Treated by Cupping Therapy
Cupping therapy effectively treated musculoskeletal pain conditions as lumbar disc herniation, cervical spondylosis, [26] brachialgia paraesthetica nocturna, [27] persistent non-specific low back pain, [28] fibrositis,[29] firomyalgia, [30] chronic non-specific neck pain,31 chronic knee osteoarthritis [32] and other pain conditions e.g. pain of dysmenorrhea [33] and pain of acute gouty arthritis [34].
Recently, we reported Al-hijamah as a suggested novel treatment for percutaneous excretion of iron and ferritin for treating thalassemia, hemochromatosis and other conditions of iron overload [35].
Cupping therapy effectively treated neurological conditions as headache and migraine, [15] acute trigeminal neuralgia [36] and carpal tunnel syndrome [37].
Cupping therapy was also effective in treating metabolic conditions e.g. acute gouty arthritis, [34]hyperlipidemia and hypercholesterolemia. [38] Cupping therapy was effective in treating respiratory diseases e.g. allergic rhinitis, [39] asthma [24] and asthmatic bronchitis [40].
Moreover, cupping therapy was effective also in treating some cardiovascular diseases e.g. systolic hypertension, [41] circulatory overload, heart failure, [42] arrhythmia, myocardial infarction (in experimental animals where WCT decreased the size of the cardiac infarct) [43].
Cupping therapy was effective in treating viral infections e.g. herpes zoster, [26] viral hepatitis [22, 23] and bacterial infections e.g. cellulitis. [17] Cupping therapy was effective in treating autoimmune diseases e.g. RA,[16] vitiligo [44] and other disease conditions e.g. secondary amenorrhoea [45] and stroke rehabilitation. [46]Cupping therapy was reported to reduce serum iron [47] and ferritin [1] in healthy subjects. Recently, Al-hijamah was reported to treat effectively some dermatological conditions e.g. acne vulgaris, chronic idiopathic urticaria and atopic dermatitis [48].
As Al-hijamah includes all steps of both Chinese DCT and WCT, therapeutic indications for performing Al-hijamah includes all diseases treated by both Chinese DCT and WCT (Table 6). All the above-mentioned therapeutic benefits of Al-hijamah (Table 4) may participate in improving the therapeutic outcome exerted by Al-hijamah in treating such disease conditions.
Table 6. Therapeutic indications of Al-hijamah (based on all therapeutic benefits of Al-hijamah)

Table 7. Evidence-based medical and scientific lessons gained from prophetic medicine regarding Al-hijamah

Table 8. Comparison between Al-hijamah and acupuncture

12. Indications and Rationales for Practicing Al-hijamah
The most important point as regard indications for practicing Al-hijamah is to understand steps of disease pathogenesis. The first question to be asked is what is the disease pathology and what are the CPS that are implicated in causing the disease process or result during its pathogenesis and to what extent does their levels increase in patient’s serum or locally at the sites of pathology?
As a golden rule, Al-hijamah is indicated whenever disease etiology and pathogenesis will improve and become corrected partially or totally from blood clearance, interstitial fluid clearance, excreting disease CPS and normalizing blood chemistry. Examples of disease conditions that may benefit from excreting excess fluids are hypertension, vascular congestion, circulatory overload and edema (whatever the etiology). Examples of diseases that may benefit from excreting excess solutes e.g. high serum iron and serum ferritin in conditions of iron overload e.g. thalassemia, sideroblastic anemia, bronze diabetes, hemosiderosis and hemochromatosis.[49, 50] In addition, common CPS for all autoimmune diseases include high serum autoantibodies, immune complexes and inflammatory mediators. [51, 52] CPS for viral infections include high serum levels of virus particles (having sizes in nanometer range), viral antigens and inflammatory mediators. [53] CPS for bacterial infections may include high serum levels of bacteria (bacteremia) and bacterial toxins (toxemia) causing secondary septicemia and septic shock. [54] CPS for musculoskeletal pain conditions include high serum and or local interstitial fluid levels of inflammatory mediators, prostaglandins, certain cytokines and pain-causing substances e.g. substance P. [55, 56] CPS for metabolic diseases include high serum levels of accumulated substrates and secondary metabolic products that may disturb organ functions. [57] CPS for hormonal imbalance e.g. endocrine hyperfunction conditions may include high serum level of hormones and or their releasing hormones, which causes secondary metabolic effects e.g. hyperestrogenemia is an etiological factor for ovulatory dysfunction causing secondary female infertility. [58] CPS for cardiovascular disorders may include hyperlipidemia and hypercholesterolemia causing secondary atherosclerosis and hypertension. [59] CPS for addiction, suicidal tendencies using drugs and drug intoxication e.g. alcoholism may include high serum levels of causative drugs with secondary metabolic deteriorations. [60] CPS for some neurological conditions may include high serum levels of causative chemical substances (DCS or DRS), inflammatory mediators, cytokines and prostaglandins. [61] For cancer patients, CPS may include high serum growth factors produced by cancer cells to facilitate malignant cell survival, progression, angiogenesis and metastasis. CPS in serum of cancer patients may include also high serum lactate dehydrogenase, lactate (Warburg effect) and tumor markers.
Lactate is a metabolic key player in cancer [62] and is reported to the mirror and motor of malignancy. [63] We and Japanese co-researchers reported that antagonizing the effects of lactate and pyruvate (through using the lactate analog, 3-bromopyruvate) killed cancer cells (glioblastoma multiforme cells), delayed their metastasis, [64] inhibited angiogenesis, [65] depleted tumor energetics, induced oxidative stress in cancer cells [66], inactivated ABC transporters (that excrete cancer chemotherapeutics) and restored drug sensitivity in malignant cells. [67] Recently, we reported that lactate produced in cancer cells (Warburg effect) increases steady-state ROS condition in cancer cells through decreasing their antioxidant capacities[68].
Al-hijamah may be beneficial for cancer patients to clear blood from those CPS (lactate, lactate dehydrogenase, cancer growth factors, metastatic growth factors and others), enhance natural immunity (anticancer effect), decrease tumor interstitial fluid pressure (an early-response marker for anticancer therapeutics [69] and potentiate therapeutic effect of chemotherapy. Clearing blood of cancer patients from lactate (Warburg effect) may deprive cancer cells from all lactate-based benefits as regard cancer cell survival, proliferation, metastasis, adhesion, invasion, angiogenesis and others. NO (endogenously produced during Al-hijamah) acts as an antiproliferative, anti-leukemia and antineoplastic agent [70].
As a golden rule, Al-hijamah is a beneficial and curative but never harmful. Degree of therapeutic benefits gained after Al-hijamah depends on the degree of response and improvement of disease pathogenesis in response to the serum clearing effect of Al-hijamah taking into account the other therapeutic benefits exerted by Al-hijamah (Table 4). Other important factors that govern the therapeutic outcomes of Al-hijamah are the skills of the practitioner (better to be physicians specialized in Al-hijamah, plastic surgeons, dermatologists or any other interested qualified licensed physicians and non-medical practitioners), number of cups, duration of cups application, optimizing suction pressure, combination with pharmacological treatment and also selecting the proper anatomical sites for cups application. Proper practice of shartat mihjam (Table 7) (Figure 5A-C) as we learnt from prophetic medicine is essential to optimize the therapeutic results of Al-hijamah. Compared with acupuncture as a traditional Chinese medicine, acupuncture needs skills for practice with some similarities and differences with Al-hijamah (Table 8).
13. Therapeutic Benefits of Al-hijamah for Diabetic and Stroke Patients
Although it was reported that the evidence for therapeutic benefits of cupping therapy as regard stroke rehabilitation is minimal, [11] this may not be applied to Al-hijamah, which has many therapeutic aspects (more than traditional DCT and WCT) that are closely related to stroke treatment in those patients. The therapeutic benefits of Al-hijamah may treat disease conditions commonly associated with stroke e.g. hypertension, hyperlipidemia, atherosclerosis [1] and may improve circulation [2, 3] e.g. to paralyzed limbs. Stroke patients are usually maintained on a long list of drugs that treat predisposing factors for stroke, especially hypertension, diabetes mellitus, hyperlipidemia, [71] vascular thrombosis (antiplatelet and anticoagulants in cerebral infarction), [72] and others. Treating the above-mentioned predisposing factors (Table 6) is as important as physiotherapy to the paralyzed muscles due to the effect of stroke. Blood clearance effect induced by Al-hijamah was reported to reduce blood pressure and improve lipid profile, [1]which is expected to delay occurrence and progression of atherosclerosis (cerebral stroke is mainly a vascular disease).
Al-hijamah may potentiate the therapeutic effects of antihypertensive and anti-hyperlipidemic drugs (drug potentiation effect) [2] and may decrease the possibility of pharmacological interactions and antagonism that may occur when many drugs are simultaneously administered. In addition, Al-hijamah may decrease the economic and financial burden upon the patient and health insurance if we could decrease the dose or frequency of concomitant drug administration. Moreover, cupping therapy (e.g. Al-hijamah) decreases vascular congestion, improves microcirculation, treats peripheral ischemia and may have a physiotherapy effect. [2, 3]Some superior effects of cupping were reported in some randomized controlled trials (compared to acupuncture) in treating hemiplegic shoulder pain and high upper-limb myodynamia after stroke. Favorable effects of cupping on aphasia and intractable hiccup after stroke were also reported [73].
As diabetes mellitus is a common association with cerebrovascular stroke, Al-hijamah may benefit patients having both diabetes and stroke despite being non-curative to diabetes mellitus itself. Al-hijamah was recently reported to decrease serum ferritin in health subjects (predisposing factor to diabetes mellitus). [1] It was recently reported that there is a significant association between high serum lipids and ferritin with the progression to insulin resistance (in type I and type II diabetes), which indicates a greater risk of micro- and macrovascular disease in diabetic patients [74, 75, 76].
Interestingly, Iron depletion improves vascular dysfunction in type-2 diabetic patients with high ferritin concentrations. [77] Hyperferritinemia may be an independent risk factor of microalbuminuria in diabetic nephropathy in patients with Type-2 diabetes. [78] Bloodletting was reported to decrease serum glycosylated hemoglobin (HbA1c) levels, to induce statistically significant increase in insulin sensitivity and to induce improvements in insulin secretion and insulin resistance that were significantly different from subjects with high-ferritin type-2 diabetes. [79] Based on that, Al-hijamah-induced non-specific pressure-dependent filtration of blood, clearance of serum ferritin and bloodletting seem to be so beneficial to guard against the development of diabetes mellitus and to treat diabetic patients (type 1 and type-2 diabetes).
Importantly, uncontrolled hyperglycemia in diabetic patients may activate the polyol pathway in which persistently high serum glucose (in uncontrolled hyperglycemia) may be converted to sorbitol (has osmotic damaging effect), may cause generation of free radicals and may induce the formation of advanced glycation end products. All those may collectively cause damage to the nerve cells and vascular endothelial cells i.e. predispose to diabetic angiopathy, neuropathy and nephropathy. [80] Unfortunately, blood chemistry of diabetic patients (uncontrolled hyperglycemia) may exhibit high serum advanced glycation end products, free radicals, metabolites of abnormal metabolism of carbohydrates and lipids (due to insulin lack), high serum cholesterol, high serum LDL and others. [80] Based on that, non-specific serum clearance induced by Al-hijamah may protect against and prevent further progression of some long-term complications of diabetes mellitus. Al-hijamah may benefit diabetic patients; prolong disease-free survival and offer better treatment outcomes. It should be considered that other therapeutic benefits of Al-hijamah e.g. enhancing immunity, neurological benefit, hemostatic benefit, homeostatic benefit and others (Table 4) may improve the general condition of diabetic and stroke patients.
Interestingly, Al-hijamah may confer some therapeutic benefits similar to that exerted by many drugs e.g. vasodilator effect (Al-hijamah treats ischemia through release of NO), [2, 12, 13] antihypertensive effect (Al-hijamah decreases both systolic and diastolic blood pressure), [1] hypolipidemic effect (Al-hijamah decreases serum triglycerides, total cholesterol and LDL-cholesterol) [1], immunostimulant effect (Al-hijamah enhances natural immunity), [16] iron-lowering effect (Al-hijamah reduces serum ferritin [1] while excessive WCT causes iron deficiency), [20, 21, 47] excretory effect to bacteria and toxins in blood (CT treats cellulitis), [17] analgesic effect (treats headache, migraine [35] and releases endogenous opioids), [2, 3] angiogenic effect (improves capillary circulation), [2, 3] urate clearance effect (Al-hijamah reduced uric acid), [1] anti-neoplastic effect (Al-hijamah clears blood chemistry of cancer patients from growth factors and cancer-related products in addition to the role of released NO). [2, 3, 70] Interestingly, there is no chance for occurrence of antagonism among those pharmacological effects of Al-hijamah with different pharmacological treatments as Al-hijamah is a mechanical procedure where no chemical interaction will develop.
14. Lessons gained from prophetic medicine regarding timing and practice of Al-hijamah
Prophetic medicine (related to Prophet Muhammad peace be upon him) recommends Al-hijamah: “The best among what you use in therapy is Al-hijamah (prophetic method of cupping therapy)” [81] and “If there is a benefit in any of your treatment modalities, benefit will be in shartat mihjam, a gulp of honey and cauterizing, but I do not like cauterization”. [82] Recently, Loukas et al. reported that knowledge gained from studying the Qur'an (spoken word of God) and Hadeeth (spoken word of Prophet Muhammad peace be upon him) enabled a good comprehension of studying some parts of the human body e.g. the heart and cardiovascular system. They reported also that remedies mentioned in prophetic medicine have agreement with modern medical knowledge. [6] When reviewing prophetic medicine as regard the practice of Al-hijamah, we can get the most important lessons regarding the procedure (shartat mihjam) (Figure 5), anatomical sites, timing and indications of Al-hijamah. We can learn also and associated treatments to be used with Al-hijamah e.g. oral honey, costus and others. In prophetic medicine, Al-hijamah is recommended in days number 17th, 19th, 21stof the lunar month (during the third quarter of the lunar month).
This agrees with modern medical reports where the gravitational pull of the moon was recently reported to affect the cardiovascular functions of the human body. In healthy subjects, both systolic blood pressure (BP) and mean arterial BP were about 5 mmHg higher in the third quarter of the lunar month (15th - 21th day of the lunar month). Physical fitness index was also lower in the third and fourth quarters of lunar month. [83] Performing Al-hijamah regularly at the 3rdquarter of the lunar month may help treating the cyclic elevations in blood pressure that usually occur.
15. Side Effects and Safety Issues during Al-hijamah
Among the most important parameters when evaluating a therapeutic modality e.g. Al-hijamah is the safety issue and side effects. With regard to Al-hijamah, it is rare to encounter a side effect when the criteria for proper practice are fulfilled as we discussed in shartat mihjam (Table 7) (Figure 5). The patient must be a good candidate for Al-hijamah i.e. hemodynamically stable and with no uncontrolled bleeding or uncontrolled coagulation disorders. It is contraindicated to perform Al-hijamah in a shocked patient, severely anemic patient or in case of a recent burn with inflamed sites for cups application. However, after the acute condition improves, re-evaluation of the patient’s general condition is needed before practicing Al-hijamah where the risk/benefit ratio should be applied. Strict sterilization is a must during the whole procedure. The triple S steps (suction, scarification and suction) of Al-hijamah should be optimized. Suction should be manual using a hand-held pump (not cotton or alcohol ignition to avoid skin burns). Suction time should be 5 minutes while suction pressure should be moderate (4 maximal suction times using the hand-held pump). Shartat mihjam (Figure 5) should be superficial skin scarifications (0.1 mm in depth) confined to the skin uplifting. Shartat mihjam should be multiple, longitudinal (1-2 mm), equally distributed and productive skin scarifications. Practitioner’s skill is to do shartat mihjam rapidly to get the maximal non-specific clearance benefit induced by Al-hijamah. Any violation from these criteria is regarded as a malpractice and is expected to carry side effects.
Reported side effects were related to the malpractice of cupping therapy (traditional DCT and traditional WCT) not Al-hijamah. However, as the cupping methodology is similar in both, reported side effects should be considered and should be divided into common and rare side effects. Common side effects include bleeding (due to deep long scarification), skin bruises (due to excessive suction pressure or prolonged suction duration causing dermal capillary rupture), keloid scarring and burns (when method of suction is cotton or alcohol ignition). [84] The rare serious side effects include acquired hemophilia A (in one patient after traditional Chinese WCT due to extensive bruising which led to pending compartment syndrome of patient’s left thigh 2 days after cupping with excessive bleeding) [85].
Cupping of the cervical area in an individual case resulted in a hemorrhagic stroke caused by an acute rise in blood pressure. Other side effects due to malpractice included factitious panniculitis (in one patient who underwent traditional WCT while traveling in an airplane), reversible cardiac hypertrophy, and iron deficiency anemia (due to too frequent sessions of traditional WCT with extensive bleeding by an unqualified practitioner)[21].
16. Future of Al-hijamah
Future of Al-hijamah is promising as a vital modality of treatment directed towards clearing serum and interstitial fluids from CPS to restore physiological homeostasis. Al-hijamah carries a lot of hope in improving the therapeutic outcomes of a large number of diseases that are still of dismal prognosis. Future scientific research and published research studies are vital to put Al-hijamah in its proper position as a simple, curative and economic modality of treatment.
The early Islamic medical scholars were pioneering in practicing, teaching and writing about Al-hijamah in their medical books e.g. Al-Qanon Fi Al-Tib (The law in medicine), which is a big textbook in medicine and surgery that was written by Avicenna (Ibn Sina). That book was among the main references to humanity medicine since the beginning of XI century until the middle of XIII century. With Al-Qanon, the golden age of the Arabic medicine came to its peak. [86, 87] Avicenna described in this great textbook many details about using Al-hijamah in treating different diseases. [88, 89] Al-hijamah is now an international evidence-based medicine available for patients, hospitals, research institutions and academics worldwide for more fruitful research and investigation. Al-hijamah is not secluded to the Arabic patients or Arabic medicine. Lack of proper understanding of how Al-hijamah treats a diverse spectrum of diseases differing in etiology and pathogeneses played an important role in delaying practicing Al-hijamah as a standard official line of treatment worldwide. Taibah mechanism (Taibah theory) for scientific bases of Al-hijamah and cupping therapy explained on medical bases the detailed mechanisms of action of Al-hijamah and differentiated it from other types of cupping therapy [2, 3].
We appreciate so much that cupping therapy is practiced officially in Chinese hospitals and in some European countries. We appreciate that Al-hijamah is practiced officially in hospitals in the United Arab Emirates. We appreciate also the fruitful efforts exerted by the Saudi Mministry of Health and the National Center for Complementary and Alternative Medicine in introducing the medical education and continuous medical training on Al-hijamah as an evidence-based medicine taking into account gaining maximum benefits of the international experience in cupping therapy to optimize and standardize the practice of Al-hijamah by qualified practitioners. The Saudi National Center for Complementary and Alternative Medicine is carrying active research projects and clinical trials for treating different diseases using Al-hijamah in the official governmental hospitals in a pure medical atmosphere in Saudi Arabia (homeland of Al-hijamah and prophetic medicine) where Al-hijamah is performed by qualified well-trained and licensed physicians who got a practice license from the Saudi Commission for Health Specialties (SCFHS).
We appreciate so much the research efforts exerted by the scientific chair of prophetic medicine in Taibah University (supervised by professor Bassim Y. Sheikh) in Al-Madinah, Saudi Arabia where a well-equipped clinic for practicing Al-hijamah according to the highest academic standards was already established and is providing the health benefits for treating patients using Al-hijamah. Al-hijamah clinic in Taibah University is carrying out active research projects to meticulously endeavor and to unravel the medical and health benefits of Al-hijamah at myriad specialties. Moreover, the scientific chair of prophetic medicine in Taibah University had a big participation and fruitful research results in investigating the therapeutic benefits of natural remedies of prophetic medicine as ajwa of Aliah (date fruit of Al-madinah). [90] and nigella sativa [91].
17. Research Recommendation
It is highly recommended to encourage the practice of Al-hijamah in hospitals in a pure medical atmosphere. The anti-diabetic effects of Al-hijamah e.g. blood clearance effects from high circulating iron stores (ferritin), abnormal lipid profile, advanced glycation end products, glycosylated serum proteins and others makes it an essential line of treatment for both preventive and therapeutic purposes in agreement with the teachings of the Prophet Muhammad peace be upon him. Currently, modern societies e.g. in the western world and in Arabic countries are characterized a sedentary life style in which physical exercise e.g. walking is minimal and dependence on the welfare transportation facilities is the rule. This may facilitate the development of some diseases e.g. obesity, insulin resistance, diabetes, hyperlipidemia, atherosclerosis, hypertension, stroke and others. Moreover, daily western diet is composed of a high content of sugars, carbohydrates and saturated lipids, which may cause a diabetogenic effect. Based on that, Al-hijamah seems to be a vital and essential modality of treatment in our Arabic societies.
18. Conclusion
Al-hijamah (WCT of prophetic medicine) may be a promising treatment for increasing immunity of human body, potentiating pharmacological effects of modern drugs and clearing blood from pathological substances causing and related to pathogenesis of many diseases.
Conflict of Interest
The authors declare that there is no conflict of interest.
Acknowledgement
Our sincere thanking is offered to the helpful revisions, nice additions and corrections made by Dr. Jameel Awwad Sulami, (H.D., Researcher & Consultant in Prophetic Medicine, Doctor of Hijamatology, Holistic and Functional Medicine Specialist from Turkey). Efforts of Dr. Jameel deserve appraisal in honestly serving prophetic medicine. Indeed, Dr. Jameel offered big efforts as an advisor for this work. We are so grateful to the library of Sohag faculty of medicine, Sohag University, Egypt for providing the internet facility and helpful textbooks.
List of Abbreviations
DCS: Disease-causing substances
DCT: Dry cupping therapy
DRS: Disease-related substances
RA: Rheumatoid arthritis
SS method: Suction and scarification method
SSS method: Suction, scarification and suction
WCT: Wet cupping therapy
NOTE : Published article and and images are from the website named Science and Education Publishing From Scientific Research to Knowledge
( http://pubs.sciepub.com/ajmbr/2/2/3/ )
Salah Mohamed El Sayed (1, 2)..... Abdel-Salam Al-quliti (3, 4) ..... Hany Salah Mahmoud (5)...... Hussam Baghdadi (2) ...... Reham A. Maria (2, 6) ...... Manal Mohamed Helmy Nabo (7, 8) ..... Ahmad Hefny (5)
Department of Medical Biochemistry, Sohag Faculty of Medicine, Sohag University, Egypt
Department of Clinical Biochemistry and Molecular Medicine, Taibah Faculty of Medicine, Taibah University, Al-Madinah Al-Munawwarah, Saudi Arabia
Alternative & Complementary Medicine Administration, Al-Madinah Al-Munawwarah, Kingdom of Saudi Arabia
Consultant Pediatrician, Directorate of Health administration and Therapeutic Services, Al-Madinah Al-Munawwarah, Kingdom of Saudi Arabia
World Federation of Alternative and Complementary Medicine, Cairo Regional Headquarter, Cairo, Egypt
Department of Medical Biochemistry, Tanta Faulty of Medicine, Tanta University, Egypt
Department of Pediatrics, Sohag Teaching Hospital, Sohag, Egypt
Division of Pediatric cardiology, Department of Pediatrics, Maternity and Children Hospital, King Abdullah Medical City, Al-Madinah Al-Munawwarah, Kingdom of Saudi Arabia
References
[1] Alshowafi FK. Effect of Blood Cupping on Some Biochemical Parameter. Med. J. Cairo Univ. 2010; 78: 311-315.
In article
[2] El Sayed SM, Mahmoud HS and Nabo MMH. Medical and scientific bases of Wet Cupping Therapy (Al-Hijamah): In Light of Modern Medicine and Prophetic Medicine. Altern Integ Med. 2013; 2: 1-16.
In article
[3] El Sayed SM, Mahmoud HS and Nabo MMH. Methods of Wet Cupping Therapy (Al-Hijamah): In Light of Modern Medicine and Prophetic Medicine. Altern Integ Med. 2013; 2: 1-16.
In article
[4] Huang YL.Cupping-bloodletting therapy of Saudi Arabia and its clinical application. Zhongguo Zhen Jiu.2008; 28: 375-377.
In article
[5] Al-Jauziyah IIQ. Prophetic Medicine (Healing with the Medicine of the Prophet Peace be upon Him). Fordham University: Darussalam Publishers & Distributors. 1999. Translated by Jalal Abual Rub.
In article
[6] Loukas M, Saad Y, Tubbs RS, Shoja MM. The heart and cardiovascular system in the Qur’an and Hadeeth. Int J Cardiol. 2010; 140: 19-23.
In article CrossRef
[7] Mahmoud HS, Abou-El-Naga M, Omar NAA, El-Ghazzawy HA, Fathy YM, Nabo MMH et al. Anatomical sites for practicing Wet Cupping Therapy (Al-Hijamah): In Light of Modern Medicine and Prophetic Medicine. Altern Integ Med 2013; In press.
In article
[8] Huber R, Emerich M, Braeunig M. Cupping-is it reproducible? Experiments about factors determining the vacuum. Complement Ther Med. 2011; 19: 78-83.
In article CrossRef
[9] Kanitakis J. Anatomy, histology and immunohistochemistry of normal human skin. Eur J Dermatol. 2002; 12: 390-9.
In article
[10] Sarin H. Physiologic upper limits of pore size of different blood capillary types and another perspective on the dual pore theory of microvascular permeability. J Angiogenes Res. 2010; 2: 14.
In article CrossRef
[11] AlBedah A, Khalil M, Elolemy A, Elsubai I, Khalil A. Hijama (cupping): a review of the evidence. Article first published online: Fact. 2011; 16: 12-16
In article CrossRef
[12] Cals-Grierson MM, Ormerod AD. Nitric oxide function in the skin. Nitric Oxide. 2004; 10: 179-93.
In article CrossRef
[13] Schäffer MR, Tantry U, van Wesep RA, Barbul A. Nitric oxide metabolism in wounds. J Surg Res 1997; 71: 25-31.
In article CrossRef
[14] Fok H, Jiang B, Clapp B, Chowienczyk P. Regulation of vascular tone and pulse wave velocity in human muscular conduit arteries: selective effects of nitric oxide donors to dilate muscular arteries relative to resistance vessels. Hypertension. 2012; 60: 1220-5.
In article CrossRef
[15] Ahmadi A, Schwebel DC, Rezaei M. The efficacy of wet-cupping in the treatment of tension and migraine headache. Am J Chin Med. 2008; 36: 37-44.
In article CrossRef
[16] Ahmed SM, Madbouly NH, Maklad SS, Abu-Shady EA. Immunomodulatory effects of bloodletting cupping therapy in patients with rheumatoid arthritis. Egypt J Immunol. 2005;12:39-51.
In article
[17] Ahmed A, Khan RA, Ali AA, Ahmed M, Mesaik MA. Effect of wet cupping therapy on virulent cellulitis secondary to honey bee sting–a case report. Journal of Basic and Applied Sciences. 2011; 7: 123-125.
In article CrossRef
[18] Farahmand SK, Gang LZ, Saghebi SA, Mohammadi M, Mohammadi S, Mohammadi G, et al. The effects of wet cupping on coronary risk factors in patients with metabolic syndrome: a randomized controlled trial.Am J Chin Med. 2012; 40: 269-77.
In article CrossRef
[19] Bilal M, Khan RA, Ahmed A, Afroz A (2011) Partial evaluation of technique used in cupping therapy. Journal of Basic and Applied Sciences 7: 65-68.
In article
[20] Sohn IS, Jin ES, Cho JM, Kim CJ, Bae JH, Moon JY et al. Bloodletting-induced cardiomyopathy: reversible cardiac hypertrophy in severe chronic anaemia from long-term bloodletting with cupping. Eur J Echocardiogr. 2008; 9: 585-6.
In article
[21] Kim KH, Kim TH, Hwangbo M, Yang GY. Anaemia and skin pigmentation after excessive cupping therapy by an unqualified therapist in Korea: a case report. Acupunct Med. 2012; 30: 227-8.
In article CrossRef
[22] Al-Saedy SA, El-Hazemy MA, Hassan MI, Badawy AS, Bahr MH. Studying molecular biology of Al-hijamah in patients with hepatitis C infection (In Arabic). Al-Ijaz Al-Ilmy (Scientific miracle). 2007; 27: 28-37.
In article
[23] Badawy AE, El-Hazemy. Al-hijamah (a scientific perspective) (In Arabic). Al-Sunnah library. Cairo, Egypt. 2007: 49-59.
In article
[24] Abd al-Jawad MEM, Mohamed SA, Elsayed BA, Mohamed ANM. Evaluation of Wet Cupping Therapy (Hijama) as an Adjuvant Therapy in the Management of Bronchial Asthma. Indian Journal of Physiotherapy and Occupational Therapy - An International Journal. 2011; 5: 122-126.
In article
[25] Lauche R, Langhorst J, Dobos GJ, Cramer H. Clinically meaningful differences in pain, disability and quality of life for chronic nonspecific neck pain - A reanalysis of 4 randomized controlled trials of cupping therapy. Complement Ther Med. 2013; 21: 342-7.
In article CrossRef
[26] Cao H, Li X, Liu J (2012) An updated review of the efficacy of cupping therapy. PLoS One 7: e31793.
In article CrossRef
[27] Lüdtke R, Albrecht U, Stange R, Uehleke B. Brachialgia paraesthetica nocturna can be relieved by “wet cupping”--results of a randomised pilot study. Complement Ther Med. 2006;14: 247-253.
In article CrossRef
[28] Last AR, Hulbert K. Chronic low back pain: evaluation and management. Am Fam Physician. 2009; 79: 1067-1074.
In article
[29] Zhang HL. Blood-letting puncture and cupping therapies combined with acupuncture for treatment of 140 cases of fibrositis. J Tradit Chin Med. 2009; 29: 277-278.
In article CrossRef
[30] Cao H, Hu H, Colagiuri B, Liu J. Medicinal cupping therapy in 30 patients with fibromyalgia: a case series observation. Forsch Komplementmed 2011; 18: 122- 126.
In article CrossRef
[31] Kim JI, Kim TH, Lee MS, Kang JW, Kim KH, Choi JY et al. Evaluation of wet cupping therapy for persistent non-specific low back pain: a randomised, waiting-list controlled, open-label, parallel-group pilot trial. Trials; 12: 146-152.
In article CrossRef
[32] Teut M, Kaiser S, Ortiz M, Roll S, Binting S, et al. (2012). Pulsatile dry cupping in patients with osteoarthritis of the knee-a randomized controlled exploratory trial. BMC Complement Altern Med. 2012; 12: 184-192.
In article CrossRef
[33] Sultana A, Ur Rahman K, Farzana M, Lone A. Efficacy of hijamat bila shurt (dry cupping) on intensity of pain in dysmenorrhoea-a preliminary study. Anc Sci Life. 2012; 30: 47-50.
In article
[34] Zhang SJ, Liu JP, He KQ. Treatment of acute gouty arthritis by blood-letting cupping plus herbal medicine. J Tradit Chin Med. 2010; 30: 18-20.
In article CrossRef
[35] El Sayed SM, Abou-Taleb A, Mahmoud HS, Ahmed NS, Nabo MM Percutaneous excretion of iron (through Al-hijamah) as a novel treatment to iron overload in beta-thalassemia major, hemochromatosis and sideroblastic anemia. Med Hypothes 2013 In press.
In article
[36] Zhang Z. Observation on therapeutic effects of blood-letting puncture with cupping in acute trigeminal neuralgia. J Tradit Chin Med. 1997; 17: 272-274.
In article
[37] Michalsen A, Bock S, Lüdtke R, Rampp T, Baecker M, et al. Effects of traditional cupping therapy in patients with carpal tunnel syndrome: a randomized controlled trial. J Pain. 2009; 10: 601-608.
In article CrossRef
[38] Niasari M, Kosari F, Ahmadi A. The effect of wet cupping on serum lipid concentrations of clinically healthy young men: a randomized controlled trial. J Altern Complement Med. 2007; 13: 79-82.
In article CrossRef
[39] Zhang C. Treatment of 31 cases of allergic rhinitis with acupuncture plus moving cupping. Journal of Acupuncture and Tuina Science. 2010; 8: 93-95.
In article CrossRef
[40] Zhang CQ, Liang TJ, Zhang W. Effects of drug cupping therapy on immune function in chronic asthmatic bronchitis patients during protracted period. Zhongguo Zhong Xi Yi Jie He Za Zhi. 2006; 26: 984-7.
In article
[41] Mohammad Zarei M, Hejazi S, Javadi SA, Farahani H. The efficacy of wet cupping in the treatment of hypertension. ARYA Atherosclerosis Journal 2012, 8: 1-6.
In article
[42] Simons RJ. Cupping. Br Med J. 1924; 1: 38.
In article CrossRef
[43] Shekarforoush S, Foadoddini M. Cardiac effects of cupping: myocardial infarction, arrhythmias, heart rate and mean arterial blood pressure in the rat heart. Chin J Physiol. 2012; 55: 253-8.
In article
[44] Awad SS. Repigmentation of poliosis after epithelial grafting for vitiligo. Dermatol Surg. 2013; 39: 406-11.
In article CrossRef
[45] Parveen R. Clinical efficacy of Hijamat Bil Shurt (Wet Cupping) in the management of Ehtebas Tams Sanwi (Secondary Amenorrhoea). Thesis:
In article
[46] Lee MS, Choi TY, Shin BC, Han CH, Ernst E. Cupping for stroke rehabilitation: a systematic review. J Neurol Sci. 2010; 15; 294:70-3.
In article CrossRef
[47] Lee HJ, Park NH, Yun HJ, Kim S, Jo DY. Cupping therapy-induced iron deficiency anemia in a healthy man. Am J Med. 2008; 121: 5-6.
In article CrossRef
[48] El-Domyati M, Saleh F, Barakat M and Mohamed N. Evaluation of Cupping Therapy in Some Dermatoses. Egyptian Dermatology Online Journal. 2013; 9: 79-82.
In article
[49] McCarthy GM, Crowe J, McCarthy CJ, Eustace S, Kenny D. Hereditary hemochromatosis: a common, often unrecognized, genetic disease. Cleve Clin J Med. 2002; 69: 224-6.
In article CrossRef
[50] Marx JJ, Kartikasari AE, Georgiou NA. Can iron chelators influence the progression of atherosclerosis? Hemoglobin. 2008; 32: 123-34.
In article CrossRef
[51] McMahon M, Hahn BH. Atherosclerosis and systemic lupus erythematosus: mechanistic basis of the association. Curr Opin Immunol. 2007; 19: 633-9.
In article CrossRef
[52] Marks SD, Tullus K. Autoantibodies in systemic lupus erythematosus. Pediatr Nephrol. 2012; 27: 1855-68.
In article CrossRef
[53] Cooper NR, Nemerow GR. The role of antibody and complement in the control of viral infections. J Invest Dermatol. 1984;83(1 Suppl):121s-127s.
In article CrossRef
[54] Feldman C, Anderson R. Bacteraemic pneumococcal pneumonia: current therapeutic options. Drugs. 2011;71:131-53.
In article CrossRef
[55] Kidd BL, Urban LA. Mechanisms of inflammatory pain. Br J Anaesth. 2001; 87: 3-11.
In article CrossRef
[56] Hassanali SH, Oyoo GO. Osteoarthritis: A look at pathophysiology and approach to new treatments: EAOJ. 2011; 5: 1-7.
In article
[57] Mutoh T, Kuriyama M. Screening methods for the diagnosis of lysosomal storage disease. Nihon Rinsho. 1995; 53: 2933-7.
In article
[58] Xita N, Tsatsoulis A. Review: fetal programming of polycystic ovary syndrome by androgen excess: evidence from experimental, clinical, and genetic association studies. J Clin Endocrinol Metab. 2006; 91: 1660-6.
In article CrossRef
[59] McCrindle BW, Urbina EM, Dennison BA, Jacobson MS, Steinberger J, Rocchini AP, et al. Drug therapy of high-risk lipid abnormalities in children and adolescents: a scientific statement from the American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee, Council of Cardiovascular Disease in the Young, with the Council on Cardiovascular Nursing. Circulation. 2007; 115: 1948-67.
In article CrossRef
[60] BANKOLE A. JOHNSON UPDATE ON NEUROPHARMACOLOGICAL TREATMENTS FOR ALCOHOLISM: SCIENTIFIC BASIS AND CLINICAL FINDINGS. Biochem Pharmacol. Biochem Pharmacol. 2008 January 1; 75:34-56.
In article CrossRef
[61] Lima IV, Bastos LF, Limborço-Filho M, Fiebich BL, de Oliveira AC. Role of prostaglandins in neuroinflammatory and neurodegenerative diseases. Mediators Inflamm. 2012;2012: 946813.
In article CrossRef
[62] Hirschhaeuser F, Sattler UG, Mueller-Klieser W. Lactate: a metabolic key player in cancer. Cancer Res. 2011; 71: 6921-5.
In article CrossRef
[63] Walenta S, Mueller-Klieser WF. Lactate: mirror and motor of tumor malignancy. Semin Radiat Oncol, 2004; 14: 267-274.
In article CrossRef
[64] El Sayed SM, El-Magd RM, Shishido Y, Chung SP, Diem TH, Sakai T, et al. 3-Bromopyruvate antagonizes effects of lactate and pyruvate, synergizes with citrate and exerts novel anti-glioma effects. J Bioenerg Biomembr. 2012; 44: 61-79.
In article CrossRef
[65] El Sayed SM, El-Magd RM, Shishido Y, Yorita K, Chung SP, Tran DH, et al. D-Amino acid oxidase-induced oxidative stress, 3-bromopyruvate and citrate inhibit angiogenesis, exhibiting potent anticancer effects. J Bioenerg Biomembr. 2012; 44: 513-23.
In article CrossRef
[66] El Sayed SM, Abou El-Magd RM, Shishido Y, Chung SP, Sakai T, Watanabe H, et al. D-amino acid oxidase gene therapy sensitizes glioma cells to the antiglycolytic effect of 3-bromopyruvate. Cancer Gene Ther. 2012; 19: 1-18.
In article CrossRef
[67] Nakano A, Tsuji D, Miki H, Cui Q, El Sayed SM, Ikegame A, et al. Glycolysis inhibition inactivates ABC transporters to restore drug sensitivity in malignant cells. PLoS One. 2011;6(11):e27222.
In article CrossRef
[68] El Sayed SM, Mahmoud AA, El Sawy SA, Abdelaal EA, Fouad AM, Yousif RS, et al. Warburg effect increases steady-state ROS condition in cancer cells through decreasing their antioxidant capacities (Anticancer effects of 3-bromopyruvate through antagonizing Warburg effect). Med Hypotheses. 2013; In press.
In article CrossRef
[69] Ferretti S, Allegrini PR, Becquet MM, McSheehy PM.Tumor interstitial fluid pressure as an early-response marker for anticancer therapeutics. Neoplasia. 2009; 11: 874-81.
In article
[70] Shami PJ, Sauls DL, Weinberg JB. Schedule and concentration-dependent induction of apoptosis in leukemia cells by nitric oxide. Leukemia. 1998; 12: 1461-6.
In article CrossRef
[71] Mouradian MS, Majumdar SR, Senthilselvan A, Khan K, Shuaib A. How well are hypertension, hyperlipidemia, diabetes, and smoking managed after a stroke or transient ischemic attack? Stroke. 2002; 33: 1656-9.
In article CrossRef
[72] Sher K, Shah S, Kumar S. Etiologic patterns of ischaemic stroke in young adults. J Coll Physicians Surg Pak. 2013;23: 472-5.
In article
[73] Lee MS, Choi TY, Shin BC, Kim JI, Nam SS. Cupping for hypertension: a systematic review. Clin Exp Hypertens. 2010; 32: 423-5.
In article CrossRef
[74] Amiri FN, Basirat Z, Omidvar S, Sharbatdaran M, Tilaki KH, Pouramir M. Comparison of the serum iron, ferritin levels and total iron-binding capacity between pregnant women with and without gestational diabetes. J Nat Sci Biol Med. 2013; 4: 302-305.
In article CrossRef
[75] Sun L, Zong G, Pan A, Ye X, Li H, Yu Z, et al. Elevated plasma ferritin is associated with increased incidence of type 2 diabetes in middle-aged and elderly chinese adults. J Nutr. 2013; 143: 1459-65.
In article CrossRef
[76] Bulum T, Duvnjak L. Insulin resistance in patients with type 1 diabetes: relationship with metabolic and inflammatory parameters. Acta Clin Croat. 2013; 52: 43-51.
In article
[77] MANUEL J, REAL F, ARROJA GP, CASTRO A, GARCIA-BRAGADO F and RICART W: Bloodletting in high-ferritin type 2 diabetes. J. American Diabetes Association. 2001; 51: 1000-1004.
In article
[78] Hsu YH, Huang MC, Chang HY, Shin SJ, Wahlqvist ML, Chang YL, et al. Association between serum ferritin and microalbuminuria in Type 2 diabetes in Taiwan. Diabet Med. 2013; 30: 1367-73
In article CrossRef
[79] Fernández-Real JM, Peñarroja G, Castro A, García-Bragado F, Hernández-Aguado I, Ricart W. Bloodletting in high-ferritin type 2 diabetes: effects on insulin sensitivity and beta-cell function. Diabetes. 2002; 51: 1000-4.
In article CrossRef
[80] Karasu C. Glycoxidative stress and cardiovascular complications in experimentally-induced diabetes: effects of antioxidant treatment. Open Cardiovasc Med J. 2010; 4: 240-56.
In article CrossRef
[81] Al-Albani (2007) Sahih and daeef sonan Abo Dawood, Book of medicine. Hadeeth number 3857, Dar Al-Maarif library, Riyadh, Saudi Arabia.
In article
[82] Al-Bukhari MI. The English Translation of Sahih Al Bukhari with the Arabic Text (9 Volume Set). Translated by Muhammad Muhsin Khan, Al-Saadawi Publications, 1996, Book 71, hadeeth 584.
In article
[83] Chakraborty U, Ghosh T. A study on the physical fitness index, heart rate and blood pressure in different phases of lunar month on male human subjects. Int J Biometeorol. 2013; 57: 769-74.
In article CrossRef
[84] Xu S, Wang L, Cooper E, Zhang M, Manheimer E, Berman B, Shen X, Lao L. Adverse events of acupuncture: a systematic review of case reports. Evid Based Complement Alternat Med. 2013; 2013: 581203.
In article CrossRef
[85] Weng YM, Hsiao CT. Acquired hemophilia A associated with therapeutic cupping. Am J Emerg Med. 2008 Oct; 26(8): 970.e1-2.
In article
[86] Masic I. On occasion of 800th anniversary of birth of Ibn al-Nafis--discoverer of cardiac and pulmonary circulation. Med Arh. 2010; 64(5): 309-13.
In article CrossRef
[87] Shoja MM, Rashidi MR, Tubbs RS, Etemadi J, Abbasnejad F, Agutter PS. Legacy of Avicenna and evidence-based medicine. Int J Cardiol. 2011 Aug 4; 150(3): 243-6.
In article CrossRef
[88] Rahman SZ, Khan RA, Latif A. Importance of pharmacovigilance in Unani system of medicine. Indian J Pharmacol. 2008. 40(Suppl 1): S17-20.
In article
[89] Kaadan AN. bone fracture in ibn sina medicine. Pan Arab J Orth Traum 2000; 4(2): 151-156.
In article
[90] Ragab AR, Elkablawy MA, Sheik BY, Baraka HN. Antioxidant and Tissue-Protective Studies on Ajwa Extract: Dates from Al-Madinah Al-Monwarah, Saudia Arabia. J Environ Anal Toxicol.
In article
[91] Abdelwahab SI, Sheikh BY, Taha MM, How CW, Abdullah R, Yagoub U, El-Sunousi R, Eid EE. Thymoquinone-loaded nanostructured lipid carriers: preparation, gastroprotection, in vitro toxicity, and pharmacokinetic properties after extravascular administration. Int J Nanomedicine. 2013; 8: 2163-72.
In article CrossRef
[92] Hekmatpou D, Moeini L, Haji-Nadali S. The effectiveness of wet cupping vs. venesection on arterial O2 saturation level of cigarette smokers: A randomized controlled clinical trial. Pak J Med Sci. 2013 Nov-Dec; 29(6): 1349-1353.
In article CrossRef
[93] Han JS. Acupuncture and endorphins. Neurosci Lett. 2004; 361: 258-261.
In article CrossRef
[94] Tian H, Tian YJ, Wang B, Yang L, Wang YY, Yang JS. Impacts of bleeding and cupping therapy on serum P substance in patients of postherpetic neuralgia. Zhongguo Zhen Jiu. 2013 Aug; 33(8): 678-81.
In article
[95] Green D, McMahon B, Foiles N, Tian L. Measurement of hemostatic factors in EDTA plasma. Am J Clin Pathol. 2008;130: 811-815.
In article CrossRef
[96] Hong SH, Wu F, Lu X, Cai Q, Guo Y. Study on the mechanisms of cupping therapy. Zhongguo Zhen Jiu. 2011; 31: 932-4.
In article
[97] Barak O, Treat JR, James WD. Antimicrobial peptides: effectors of innate immunity in the skin. Adv Dermatol. 2005; 21: 357-374.
In article CrossRef
[98] Bassaneze V, Barauna VG, Lavini-Ramos C, Kalil J, Schettert IT, Miyakawa AA, et al. Shear stress induces nitric oxide-mediated vascular endothelial growth factor production in human adipose tissue mesenchymal stem cells. Stem Cells Dev. 2010; 19: 371-8.
In article CrossRef
[99] Akbari A, Zadeh SM, Ramezani M, Zadeh SMS. The Effect of Hijama (Cupping) on Oxidative Stress Indexes & various Blood Factors in Patients Suffering from Diabetes Type II.
In article
[100] Arslan M, Yeşilçam N, Aydin D, Yüksel R, Dane S. Wet cupping therapy restores sympathovagal imbalances in cardiac rhythm. J Altern Complement Med. 2014 Apr; 20(4): 318-21.
In article CrossRef
[101] Al-Albani (2007) Sahih and daeef sonan Abo Dawood, Book of medicine. Hadeeth number 3863, Dar Al-Maarif library, Riyadh, Saudl Arabia.
In article
[102] Al-Bukhari MI (1996) The English Translation of Sahih Al Bukhari with the Arabic Text (9 Volume Set). Translated by Muhammad Muhsin Khan, Al-Saadawi Publications, Book of medicine, chapter of Al-hijamah for headache and migraine. hadeeth no. 5701.
In article
[103] Al-Albani (2008) Sahih and daeef sonan Ibn Majah. Hadeeth no. 3483. Book of medicine. Dar Al-Maarif library, Riyadh, Saudi Arabia.
In article
[104] Al-Albani (2008) Sahih and daeef sonan Ibn Majah. Hadeeth no. 2163-2164. Book of medicine. Dar Al-Maarif library, Riyadh, Saudi Arabia.
In article
[105] Al-Nasaee AS (2008). Al-sonan Al-kobra (Great sonan). Book of medicine. Chapter of Al-hijamah. Hadeeth no. 7550. Dar Al-Maarif library, Riyadh, Saudi Arabia.
In article
[106] Al-Albani (2008) Sahih and daeef sonan Ibn Majah. Book of medicine. Chapter of (which are the days of Al-hijamah?). Hadeeth no. 3486. Dar Al-Maarif library, Riyadh, Saudi Arabia.
In article
[107] Swartz MN, Pasternack MS. Principles and Practice of Infectious Diseases. In: Cellulitis and subcutaneous tissue infections. GL Mandell et al., (6th edn) Elsevier Churchill Livingstone, Philadelphia. 2005. pp 1178-1180.
In article
[108] Messlinger K, Fischer MJ, Lennerz JK. Neuropeptide effects in the trigeminal system: pathophysiology and clinical relevance in migraine. Keio J Med. 2011; 60: 82-89.
In article CrossRef
[109] Al-Bukhari MI. The English Translation of Sahih Al Bukhari. Book of medicine. Chapter of (Cure is in three). Hadeeth numbers 5680-5681. Assryia library, Sayda, Lebanon 2002.
In article
[110] Bouwstra JA, Honeywell-Nguyen PL, Gooris GS, Ponec M. Structure of the skin barrier and its modulation by vesicular formulations. Prog Lipid Res. 2003 Jan; 42(1): 1-36. Review.
In article CrossRef
[111] Tsuchiya M, Sato EF, Inoue M, Asada A. Acupuncture enhances generation of nitric oxide and increases local circulation. Anesth Analg. 2007 Feb; 104(2): 301-7.
In article CrossRef
[112] Schäffer MR, Tantry U, van Wesep RA, Barbul A.Nitric oxide metabolism in wounds. J Surg Res. 1997 Jul 15; 71(1): 25-31.
In article CrossRef
[113] Kamaratos AV, Tzirogiannis KN, Iraklianou SA, Panoutsopoulos GI, Kanellos IE, Melidonis AI. Manuka honey-impregnated dressings in the treatment of neuropathic diabetic foot ulcers. Int Wound J. 2012 Sep 18.
In article CrossRef
[114] Al-Waili NS, Salom K, Butler G, Al Ghamdi AA. Honey and microbial infections: a review supporting the use of honey for microbial control. J Med Food. 2011 Oct; 14(10): 1079-96.
In article CrossRef
[115] Al-Albani (2008) Sahih and daeef sonan Ibn Majah. Book of medicine. Chapter of (which are the days of Al-hijamah?). Hadeeth no. 3487. Dar Al-Maarif library, Riyadh, Saudi Arabia.
In article
[116] Eliza J, Daisy P, Ignacimuthu S, Duraipandiyan V. Antidiabetic and antilipidemic effect of eremanthin from Costus speciosus (Koen.)Sm., in STZ-induced diabetic rats. Chem Biol Interact. 2009; 182: 67-72.
In article CrossRef
[117] Al-Albani (2008) Sahih and daeef sonan Al-termini. Book of medicine of Prophet Muhammad peace be upon him. Chapter of (What was narrated in Al-hijamah). Hadeeth no. 2051. Dar Al-Maarif library, Riyadh, Saudi Arabia.
In article
[118] Adams D, Cheng F, Jou H, Aung S, Yasui Y, Vohra S. The safety of pediatric acupuncture: a systematic review. Pediatrics. 2011 Dec; 128(6): e1575-87.
In article
[119] Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008 Aug; 85(4): 355-75.
In article CrossRef
[120] Ceccherelli F, Rigoni MT, Gagliardi G, Ruzzante L. Comparison of superfi cial and deep acupuncture in the treatment of lumbar myofascial pain: a double-blind ran- domized controlled study. Clin J Pain 2002; 18: 149-53.
In article CrossRef
[121] Johnstone PA, Polston GR, Niemtzow RC, Martin PJ. Integration of acupuncture into the oncology clinic. Palliat Med 2002; 16: 235-9.
In article CrossRef
[122] Bullock ML, Kiresuk TJ, Sherman RE, Lenz SK, Culliton PD, Boucher TA, et al. A large randomized placebo-controlled study of auricular acupuncture for alcohol dependence. J Subst Abuse Treat 2002; 22: 71-7.
In article CrossRef
[123] Dong H, Ludicke F, Comte I, Campana A, Graff P, Bischof P. An exploratory pilot study of acupuncture on the quality of life and reproductive hormone secretion in menopausal women. J Altern Complement Med 2001; 7: 651-8.
In article CrossRef
[124] Loyeung BY, Cobbin DM. Investigating the effects of three needling parameters (manipulation, retention time, and insertion site) on needling sensation and pain profiles: a study of eight deep needling interventions. Evid Based Complement Alternat Med. 2013; 2013: 136763.
In article
[125] Ernst E. Acupuncture--a critical analysis. J Intern Med. 2006 Feb; 259(2): 125-37.
In article CrossRef
[126] Madsen MV, Gøtzsche PC, Hróbjartsson A. Acupuncture treatment for pain: systematic review of randomised clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ. 2009 Jan 27; 338: a3115.
In article CrossRef
[127] Lee MS, Ernst E. Acupuncture for pain: an overview of Cochrane reviews. Chin J Integr Med. 2011 Mar; 17(3): 187-9.
In article CrossRef
[128] Hsiang-Tung C. Neurophysiological basis of acupuncture analgesia. Sci Sin. 1978 Nov-Dec; 21(6): 829-46.
In article
[129] Williams WF (2013). Encyclopedia of Pseudoscience: From Alien Abductions to Zone Therapy. Routledge. p. 3.
In article
[130] Ulett GA (2002). "Acupuncture". In Shermer, M. The Skeptic: Encyclopedia of Pseudoscience. ABC-CLIO. pp. 283-91.
In article
[131] Cao X. Scientific bases of acupuncture analgesia. Acupunct Electrother Res. 2002; 27(1): 1-14.
In article
[132] Chung A, Bui L, Mills E. Adverse effects of acupuncture. Which are clinically significant? Can Fam Physician. 2003 Aug; 49: 985-9.
In article
[133] Hicks A. The acupuncture handbook: how acupuncture works and how it can help you. Piatkus Books, 2005, p. 41.
In article
[134] Collinge WJ. (1996). The American Holistic Health Association Complete guide to alternative medicine. New York: Warner Books.
In article
[135] Taylor P, Pezzullo L, Grant SJ, Bensoussan A. (2013). "Cost-effectiveness of Acupuncture for Chronic Nonspecific Low Back Pain". Pain Practice: The Official Journal of World Institute of Pain.
In article
[136] Drivdahl CE, Miser WF. The use of alternative health care by a family practice population. J Am Board Fam Pract 1998; 11: 193-9.
In article CrossRef
[137] Verhoef MJ, Sutherland LR. General practitioners’ assessment of and interest in alternative medicine in Canada. Soc Sci Med 1995; 41: 511-5.
In article CrossRef
[138] Zaza C, Sellick SM, Willan A, Reyno L, Browman GP. Health care profession- als’ familiarity with non-pharmacological strategies for managing cancer pain. Psychooncology 1999;8:99-111.
In article CrossRef
[139] Lao L, Bergman S, Hamilton GR, Langenberg P, Berman B. Evaluation of acupuncture for pain control after oral surgery: a placebo-controlled trial. Arch Otolaryngol Head Neck Surg 1999; 125: 567-72.
In article CrossRef
[140] Wang B, Tang J, White PF, Naruse R, Sloninsky A, Kariger R, et al. Effect of the intensity of transcutaneous acupoint electrical stimulation on the postoperative analgesic requirement. Anesth Analg 1997; 85: 406-13.
In article
[141] British Medical Acupuncture Society. Warrington, UK. Available at: http:// www.medical-acupuncture.co.uk/about.shtml. Accessed 2003 May 28.
In article













Comments